
GLP-1 receptor agonists alter eating behavior by suppressing appetite, increasing satiety, and reshaping food preferences through hormonal and neurological pathways. Glucagon-like peptide-1 (GLP-1) is a naturally occurring gut hormone that signals fullness to your brain after eating. Medications like semaglutide and tirzepatide mimic this hormone at much higher concentrations, producing effects that go well beyond what your body generates on its own. Understanding how GLP-1 changes eating behavior explains why these treatments produce such consistent weight loss results across diverse patient populations.
What biological mechanisms cause GLP-1 to alter eating behavior?
GLP-1 receptor agonists work through a dual-action mechanism that combines physical and neurological effects to reduce food intake. No other class of weight loss medication targets both systems simultaneously with this level of clinical consistency.
The physical side of the equation starts in your gut. GLP-1 medications slow gastric emptying, which means food stays in your stomach longer after each meal. That extended presence sends continuous fullness signals through the vagus nerve to your brainstem. The result is smaller meals and longer gaps between eating without requiring willpower or calorie counting.
The neurological side is where GLP-1 gets particularly interesting. GLP-1 receptors are present in the hypothalamus and brainstem, two brain regions that directly regulate hunger and energy balance. When activated, these receptors reduce the release of hunger-promoting signals and amplify satiety signals. This is why patients on semaglutide often report that hunger simply stops feeling urgent.
Beyond hunger reduction, GLP-1 blunts reward-related brain activity in the insula, a region associated with food motivation. This distinction matters: GLP-1 reduces your wanting of food without eliminating your enjoyment of it. You can still find a meal satisfying. You just stop being driven toward food by compulsive urges.
- GLP-1 receptors are located in the gut, pancreas, vagus nerve, hypothalamus, and brainstem
- Slowed gastric emptying prolongs physical fullness after meals
- Hypothalamic signaling reduces hunger hormone activity
- Reward pathway modulation in the insula lowers food-seeking motivation
- The combined effect reduces both caloric intake and the psychological drive to eat
Pro Tip: If you are new to GLP-1 therapy, track your hunger levels on a simple 1–10 scale before and after meals during the first four weeks. This gives you concrete data on how the medication is shifting your appetite baseline, which helps you and your provider fine-tune dosing.
How does GLP-1 treatment change food preferences and eating patterns?
GLP-1 therapy does not just make you eat less. It changes what you want to eat and how you eat it. This shift in food preference is one of the most clinically significant and underreported effects of treatment.
Semaglutide treatment over six months significantly reduced total eating behavior scores across motives, way of eating, and dietary content in study participants. That breadth of change across multiple behavioral domains is unusual for a single medication. It suggests GLP-1 is not simply suppressing appetite but reorganizing the entire relationship a person has with food.
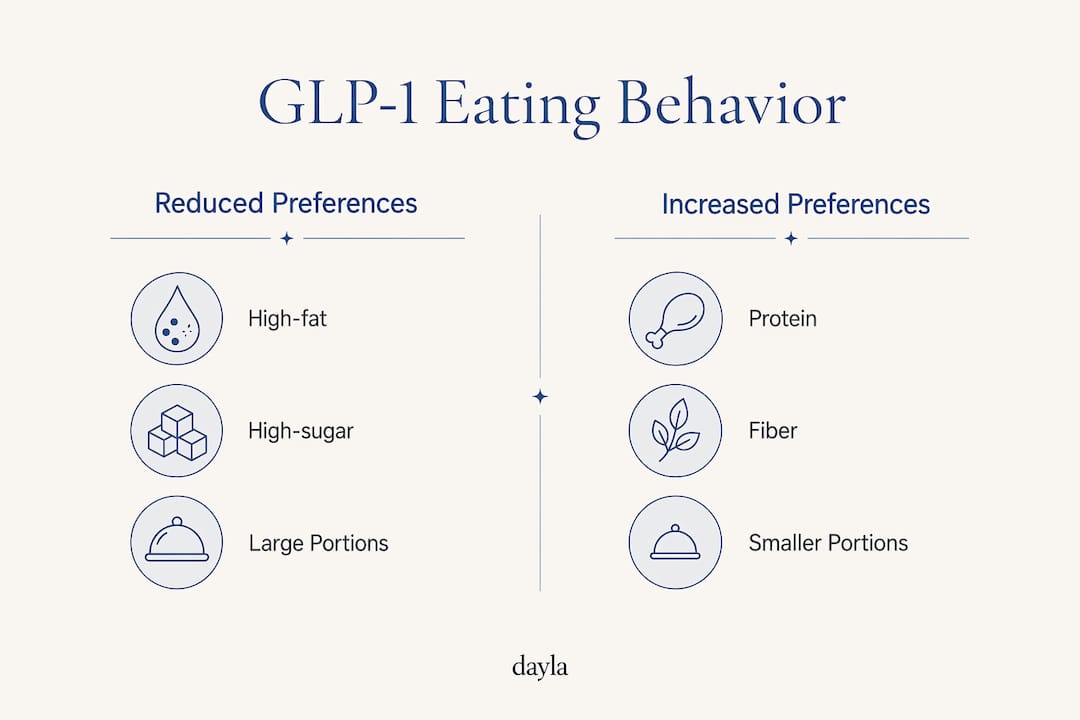
The most consistent dietary shift is a reduced preference for high-fat and high-sugar foods. GLP-1 medications shift food preferences toward less calorie-dense options, with patients spontaneously choosing foods higher in protein and fiber. This is not a conscious dietary decision. It is a biological recalibration.
| Food category | Typical change during GLP-1 therapy |
|---|---|
| High-fat foods (fried, processed) | Reduced preference and consumption |
| High-sugar foods (sweets, soda) | Reduced cravings and intake |
| Protein-rich foods (meat, eggs, legumes) | Preference maintained or increased |
| Fiber-rich foods (vegetables, whole grains) | Preference maintained or increased |
| Portion sizes overall | Consistently smaller across all food types |
Behavioral patterns shift alongside food preferences. Patients report lower impulsivity around food, meaning they are less likely to eat in response to external cues like seeing an advertisement or smelling food in a restaurant. Meal timing also becomes more deliberate. Many patients naturally move toward two or three structured meals per day rather than frequent snacking.
- Reduced impulsive eating in response to visual or environmental food cues
- More consistent meal timing with fewer unplanned snacks
- Smaller portions at each sitting without conscious restriction
- Spontaneous shift toward protein and fiber over refined carbohydrates and fats
For practical guidance on adjusting your meals to match these changes, the GLP-1 meal planning guide at Daylahealth covers specific strategies for eating well on a reduced appetite.
What are the nuanced effects of GLP-1 on food cravings and emotional eating?
GLP-1 therapy produces a well-documented reduction in food cravings, but the mechanism behind it is more specific than most people realize. The medication targets the wanting side of food reward, not the liking side. That distinction has real implications for how you experience treatment.
The concept of "food noise" captures this effect well. Food noise refers to the constant, intrusive thoughts about food that many people with obesity experience throughout the day. Patients report psychological relief from reduced food preoccupations during GLP-1 treatment, describing the experience as mental quiet they had not felt in years. This relief is not trivial. For many patients, it is the most life-changing aspect of therapy.
"The constant mental chatter about food just stopped. I wasn't thinking about my next meal while eating my current one." This type of patient report is consistent across qualitative studies on GLP-1 therapy and reflects the medication's effect on reward pathway activity in the brain.
Emotional eating is a more complicated story. GLP-1 medications reduce food cue reactivity and external eating behaviors, but they do not consistently resolve mood-driven eating. A patient who eats in response to stress, anxiety, or boredom may see only partial improvement. The biological drive to eat decreases, but the emotional trigger remains intact.
This is why behavioral support remains a critical component of GLP-1 therapy. Cognitive behavioral strategies, structured meal planning, and regular check-ins with a care team address the emotional layer that medication alone cannot fully reach.
Pro Tip: If you notice that stress or boredom still triggers eating urges despite reduced physical hunger on GLP-1 therapy, that is a signal to add behavioral support to your treatment plan. The medication handles the biology. You still need tools for the psychology.
How do GLP-1 eating behavior changes support sustainable weight loss?
The behavioral and biological changes produced by GLP-1 therapy work together to create a calorie deficit that is easier to maintain than traditional dieting. This is the core reason these medications produce superior long-term weight loss outcomes compared to lifestyle intervention alone.
- Smaller meal sizes reduce total caloric intake at each eating occasion without requiring active restriction or calorie tracking.
- Longer intervals between meals lower overall daily calorie consumption by reducing snacking and opportunistic eating.
- Shifted food preferences toward protein and fiber improve dietary quality, which supports satiety and preserves lean muscle mass during weight loss.
- Reduced food cue reactivity lowers the frequency of unplanned eating events that typically derail weight loss efforts.
- Improved insulin sensitivity complements calorie reduction by improving how your body processes the food you do eat.
The metabolic benefits extend beyond appetite. GLP-1 agonists like semaglutide reduce LDL cholesterol by 3–8% and triglycerides by 15–30%, improving cardiovascular risk alongside weight loss. These lipid improvements are linked to reduced liver fat and better insulin function, not just lower calorie intake. Tirzepatide, a dual GIP-GLP-1 receptor agonist, produces superior effects on cholesterol and triglycerides compared to conventional GLP-1 agonists, making it a strong option for patients with both obesity and metabolic risk factors.
| Outcome | Mechanism driving it |
|---|---|
| Reduced calorie intake | Smaller portions, longer meal gaps, lower cravings |
| Improved dietary quality | Spontaneous shift toward protein and fiber |
| Better blood sugar control | Enhanced insulin secretion and sensitivity |
| Lower LDL and triglycerides | Reduced hepatic fat, improved lipid metabolism |
| Sustained weight loss | Combined behavioral and metabolic effects |
Combining GLP-1 therapy with lifestyle changes that boost results produces significantly better outcomes than medication alone. Exercise, sleep quality, and stress management each amplify the appetite-regulating effects of GLP-1 and help preserve the weight loss achieved during treatment.
Key takeaways
GLP-1 receptor agonists change eating behavior through a dual mechanism: slowing gastric emptying to extend physical fullness and modulating brain reward pathways to reduce the motivation to eat.
| Point | Details |
|---|---|
| Dual-action appetite control | GLP-1 slows stomach emptying and reduces brain hunger signals simultaneously. |
| Food preference shifts | Patients spontaneously reduce high-fat and high-sugar intake while maintaining protein and fiber consumption. |
| Food noise reduction | GLP-1 therapy quiets intrusive food thoughts, providing psychological relief that supports behavior change. |
| Emotional eating limits | GLP-1 reduces external food cue reactivity but does not consistently resolve mood-driven eating. |
| Metabolic benefits | Semaglutide reduces LDL cholesterol by 3–8% and triglycerides by 15–30%, complementing weight loss outcomes. |
Why GLP-1 therapy is more than just appetite suppression
I have reviewed a lot of patient experiences and clinical data on GLP-1 therapy, and the thing that stands out most is how often people underestimate what they are getting into. Not in a negative sense. They underestimate how fundamentally this medication changes their relationship with food.
Most people expect to feel less hungry. They do not expect to stop thinking about food constantly. They do not expect to look at a plate of fries and feel genuinely indifferent. That shift in food psychology is real, and it is backed by solid neurobiological evidence. But it also creates a risk: patients sometimes assume the medication is doing all the work, so they stop paying attention to their eating patterns.
The patients who get the best long-term results are the ones who use the reduced appetite as an opportunity to build better habits, not just eat less of the same things. They track their progress, adjust their meal composition, and address the emotional eating patterns that GLP-1 does not fully resolve. The medication gives you a window. What you do with that window determines whether the results last.
One more thing worth saying directly: GLP-1 side effects like nausea and gastrointestinal discomfort are real and can temporarily distort your eating patterns in ways that feel like progress but are actually just avoidance. Eating less because you feel nauseated is not the same as eating less because your appetite is regulated. Know the difference, and work with your care team to manage side effects properly.
— Flexible
Start your GLP-1 journey with Daylahealth
If you are ready to experience how GLP-1 changes eating behavior for yourself, Daylahealth offers doctor-led, personalized GLP-1 care designed around your specific weight loss goals. Treatment plans include medication, ongoing clinical support, and practical guidance on nutrition and lifestyle adjustments that maximize your results.
Daylahealth connects you with licensed providers who understand the full picture of GLP-1 therapy, from appetite regulation to metabolic health. You get more than a prescription. You get a structured plan that addresses the behavioral and biological sides of weight loss together. Visit the GLP-1 treatment page to review your options, complete a brief intake assessment, and take the first step toward doctor-supervised care that works.
FAQ
How does GLP-1 reduce hunger?
GLP-1 receptor agonists slow gastric emptying and activate appetite-regulating centers in the hypothalamus and brainstem, producing both physical fullness and reduced hunger signaling. The combined effect means you feel full sooner and stay full longer after each meal.
Does GLP-1 change what foods you crave?
Yes. GLP-1 therapy consistently shifts food preferences away from high-fat and high-sugar foods toward protein and fiber-rich options. This change is biological rather than intentional, driven by altered reward pathway activity in the brain.
What is "food noise" and does GLP-1 stop it?
Food noise refers to the constant, intrusive thoughts about food that many people experience throughout the day. GLP-1 therapy significantly reduces these preoccupations, with patients describing the effect as mental quiet that supports better food control.
Does GLP-1 help with emotional eating?
GLP-1 medications reduce external food cue reactivity but do not consistently resolve emotional eating driven by stress, anxiety, or boredom. Behavioral support strategies remain important for patients whose eating is mood-dependent.
How does GLP-1 affect blood sugar and cholesterol?
GLP-1 receptor agonists improve insulin sensitivity and stimulate insulin secretion in response to meals, directly improving blood sugar control. Semaglutide also reduces LDL cholesterol by 3–8% and triglycerides by 15–30%, making it beneficial for patients managing both weight and metabolic risk.